
Masticatory Muscle Myositis in
the Cavalier King Charles Spaniel
-
 What
It Is
What
It Is - Symptoms
- Diagnosis
- -- Blood Test
- Treatment
- Prognosis
- Current Research
- Related Links
- Veterinary Resources
Masticatory muscle myositis (MMM) is a neuromuscular disease in which the muscles used by the dog to chew - the jaw and temporal muscles, which are called masticatory muscles - are inflamed, and it is painful and difficult or impossible for the dog to open its mouth. Trismus is the medical term describing the inability to open the mouth, but usually is attributed to causes such as trauma to the temporomandibular joint (TMJ) or bacterial infections such as tetanus. In dogs, and particularly in the cavalier King Charles spaniel, MMM is the most common form of trismus.
What It Is
MMM is an immune-mediated disease which is reportedly hereditary in the cavalier King Charles spaniel.* In at least one case, four CKCS puppies were diagnosed with MMM at the age of 12 weeks, less than two weeks following routine vaccinations. Other breeds in which MMM is most common are German shepherds, Labrador retrievers, Doberman pinschers, and golden retrievers.
* See Masticatory Myositis (Eosinophilic Myositis).
"Myositis" is a general term for inflammation of the muscles. "Immune-mediated" diseases are conditions in which the immune system may over-react or start attacking the body. MMM has also been known as "eosinophilic myositis" or "atrophic myositis". The inability to open the mouth is called "trismus".
This condition is limited to the masticatory muscles because they have a molecular structure, called 2M muscle fibers, which are found nowhere else in the dog's body. Masticatory myositis results when the immune system's antibodies specifically target these 2M muscle fibers.
The disorder is known to have an early onset in cavalier King Charles spaniels, having occurred in cavalier littermates as young as twelve weeks of age (see 2007 study report), and several other CKCSs before six months. The reported typical age of onset is about three years
In a 2005 study, Dr. Diane Shelton, board certified in veterinary internal medicine, concluded:
"In a search of the database of the Comparative Neuromuscular Laboratory over the years 2001-2005, masticatory muscle myositis was confirmed in 11 young Cavalier King Charles Spaniels with onset at less than 6 months of age. In several cases, onset followed within 10 days of vaccinations. Although long-term information is not yet complete, there was resolution of clinical signs of masticatory muscle myositis in most cases. Of interest, other complications such as early onset hypothyroidism and allergies were reported. Additional information will be provided as more is learned about this early-onset masticatory muscle myositis in this breed."
RETURN TO TOP
Symptoms
 Masticatory muscle myositis may start suddenly or appear gradually. The main clinical sign is
difficulty in opening the mouth (called "trismus"). In the initial (acute)
stage, there may also be ptyalism (an excess production of saliva), swelling of the jaw and temporal muscles, pain in
the jaw, and bulging eyes due to the swollen muscles behind them. There may
be a fever and a swollen local lymph node. The dog will seem to in pain when
he tries to open his mouth or attempts to chew and will be reluctant to eat.
Masticatory muscle myositis may start suddenly or appear gradually. The main clinical sign is
difficulty in opening the mouth (called "trismus"). In the initial (acute)
stage, there may also be ptyalism (an excess production of saliva), swelling of the jaw and temporal muscles, pain in
the jaw, and bulging eyes due to the swollen muscles behind them. There may
be a fever and a swollen local lymph node. The dog will seem to in pain when
he tries to open his mouth or attempts to chew and will be reluctant to eat.
In a December 2019 article, a New Zealand 16-week-old cavalier, which was diagnosed with MMM, displayed a 3-day history of dysphagia, hypersalivation, lip-smacking and unwillingness to open the mouth. The puppy held it mouth slightly open at rest, and there was saliva staining of the fur around the mouth. The dog expressed signs of pain when the jaw and trismus were manipulated.
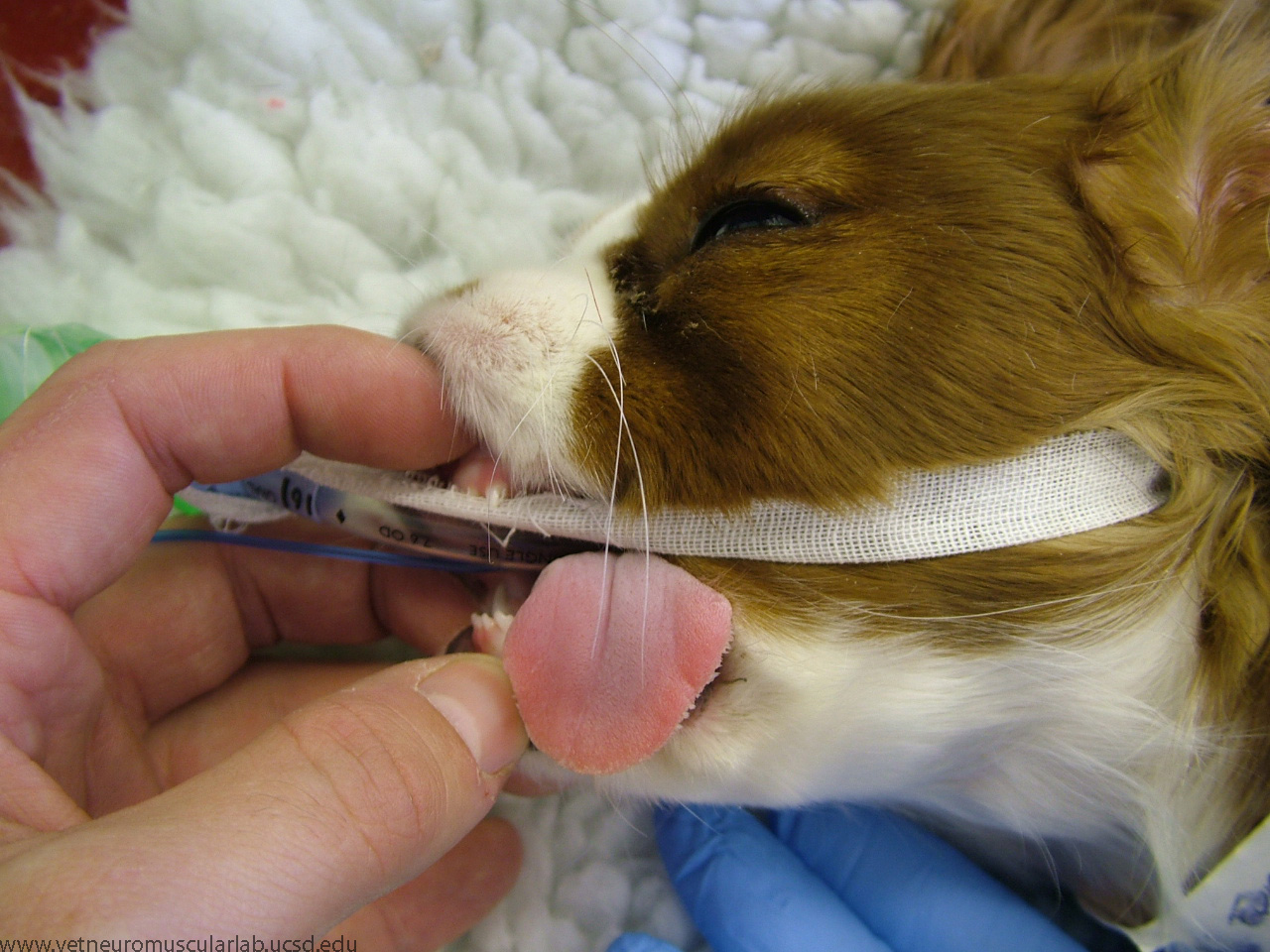
If MMM is not noticed early enough, it develops into the chronic stage, in which damaged muscle fibers are replaced with fibrotic connective tissue which results in further restriction of opening the mouth. In the chronic stage, there is noticeable atrophy of the masticatory muscles and inability to open the mouth due to the fibrosis. Instead of appearing swollen, the dog's jaw and temple muscles will hollow. The fibrosis can become so severe that the mouth cannot be opened, even under general anesthesia (see cavalier's jaw barely opened, at right) - a very serious form of lockjaw. Unfortunately, many owners do not recognize that their dogs are having a problem until they reach the chronic phase.
Some mouth symptoms are similar to those of muscular dystrophy, another neuromuscular disease affecting the mouth muscles.
RETURN TO TOP
Diagnosis
You may expect your cavalier to endure a battery of diagnostic tests, including complete physical and neurologic examinations, general and specialized blood tests - there is a unique blood test for masticatory muscle myositis called the "2M antibody" test (see box) - as well as a muscle biopsy, x-rays, urinalysis, and electromyography.
The Most Accurate Blood Test for MMM
The 2M antibody blood test detects circulating antibodies against masticatory muscles' 2M fibers. Only the masticatory muscles have the molecular structure called 2M fibers. Masticatory myositis results when the immune system's antibodies specifically target these 2M fibers.
The 2M antibody test is an "immunocytochemical" test, in which positives for MMM reportedly have been proven to be 100% accurate, and false negatives for MMM have occurred only 10% to 15% of the time. A positive result is an antibody titer of 1:500, 1:1000 or 1:4000, diagnostic of MMM.
![]() The test is conducted by the Comparative Neuromuscular Laboratory at the
University of California, San Diego. Serum samples should be sent to the
laboratory; its turn around time for reporting results is five to seven week
days. The laboratory's director is Dr. G. Diane Shelton, ACVIM board certified
in internal medicine. Contact information is on this website:
Comparative
Neuromuscular Laboratory.
The test is conducted by the Comparative Neuromuscular Laboratory at the
University of California, San Diego. Serum samples should be sent to the
laboratory; its turn around time for reporting results is five to seven week
days. The laboratory's director is Dr. G. Diane Shelton, ACVIM board certified
in internal medicine. Contact information is on this website:
Comparative
Neuromuscular Laboratory.
The purpose of some of the tests is to rule out other possible causes of the symptoms. For example, the physical and neurologic examinations are to confirm that clinical signs are limited to the masticatory muscles. Polymyositis is a more generalized muscle inflammation of the masticatory muscles and other muscles but otherwise is difficult to distinguish from masticatory myositis. Other possible causes of such symptoms include temporomandibular joint disorders, and endocrine disorders, such as Cushing's syndrome and hypothyroidism.
General anesthesia may be called for to get the dog to open its mouth to check for other possible causes of the pain, such as broken teeth or bones or a dislocated jaw. In advanced chronic cases, the dog's jaws may not open even under anesthesia.
Magnetic resonance imaging (MRI) is considered the best means for identifying MMM, allowing for early detection of the affected muscles. In a September 2013 journal article, veterinary researchers reported that magnetic resonance imaging (MRI) scanning detected "widespread, symmetrical, and inhomogeneously hyperintense areas in the masticatory muscle", enabling early diagnosis and therapeutic treatment."
If the dog's jaw or temporal muscles have started to atrophy (a symptom in the chronic stage of MMM), the examining veterinarian should find out if the dog has been treated with lengthy (seven days or longer) corticosteroid therapy for another disorder, since corticosteroids have been known to cause these muscles to atrophy.
The owner should tell the veterinarian about any recent vaccinations of the dog. Dr. Diane Shelton, board certified in veterinary internal medicine, recently reported that several young cavaliers developed MMM within ten days of vaccinations.
RETURN TO TOP
Treatment
 It is important to begin therapy of the MMM-affected dog as early as
possible, so that the acute stage does not progress to the chronic stage.
However, treatment should not begin before thorough testing and diagnosis.
It is important to begin therapy of the MMM-affected dog as early as
possible, so that the acute stage does not progress to the chronic stage.
However, treatment should not begin before thorough testing and diagnosis.
The standard course of treatment consists of heavy, lengthy doses of corticosteroids, such as prednisone (prednisolone), until the dog's jaw seems to open normally. Then, the doses may be lowered gradually over six to nine months. If the medication is discontinued too early, the dog may be expected to relapse. So, sufficient dosages of corticosteroids need to be given and for a sufficient period of time. MMM is known to respond well initially to corticosteroid therapy, but a relapse usually will occur if the treatment is discontinued prematurely. In some cases, the drug cannot ever be completely stopped.
Prednisone is a synthetic corticosteroid which serves as an "immunosuppressant" intended to suppress the dog's immune system. Prednisone may have some harmful side effects. Patients on long term prednisone will drink and urinate excessively. For dogs not able to tolerate the side effects of corticosteroids, another immunosuppressive drug, azathioprine (Azasan, Imuran, Azamun, Imurel) may be prescribed in addition to corticosteroid treatment.
Other drugs which have been considered for treatment of MMM include dexamethasone, which is approximately ten times stronger than prednisone, and cyclosporine, which is another immunosuppressive drug, and colchicine, which is used for its anti-fibrotic properties in liver disease.
The dog may require a semi-liquid diet during initial recovery. Its mouth should not be forced open, but the dog should be encouraged to chew its toys, as a form of physical therapy.
RETURN TO TOP
Prognosis
Prognosis of recovery from masticatory muscle myositis is determined by the degree of fibrosis present and the dog's response to treatment. The prognosis is good if: (a) MMM is detected early, in the initial "acute" stage; and (b) the treatment is appropriate, meaning mainly aggressive immunosuppressive therapy comprised of high doses of medication given long enough to avoid a relapse. "Good" prognosis means that a full or significant partial range of jaw motion is regained.
 Dogs which are not treated until they are in the "chronic" stage of
masticatory muscle myositis may be expected to have a less favorable prognosis.
The young cavalier at the left has suffered atrophy of both of his masticatory
muscles due to MMM. (Photo from Platt & Garosi, "Small Animal Neurological
Emergencies".)
Dogs which are not treated until they are in the "chronic" stage of
masticatory muscle myositis may be expected to have a less favorable prognosis.
The young cavalier at the left has suffered atrophy of both of his masticatory
muscles due to MMM. (Photo from Platt & Garosi, "Small Animal Neurological
Emergencies".)
However, with MMM, the treatment may turn out to be worse than the disease itself. Some dogs cannot tolerate the prescribed drugs, particularly the corticosteroids. At least one cavalier being treated for MMM is known to have suffered a slow death from the medications.*
*Read Butter's experience with MMM and its treatment.
RETURN TO TOP
Current Research
October 2022:
Cavalier puppy is successfully treated for masticatory muscle
myositis.
 In
a
September 2022 article, Italian clinicians (Martin Di Tosto,
Carolina Callegari, Kaspar Matiasek, Giuseppe Lacava, Giovanna
Salvatore, Sara Muñoz Declara, Barbara Betti, Federica Tirrito
[right]) report the case study of a 5-month-old male cavalier King
Charles spaniel (in photo below) with an inability to close his
jaw, along with lethargy and difficulty holding food in his mouth
(prehension). He could not close his mouth without assistance, and also
an inability to open his jaw. He also suffered jaw pain, inability to
fully close his eyelids, and atrophy of his masticatory (temporal and
masseter) muscles. In addition to several blood tests and a needle
aspiration of lymph nodes, to eliminate other causes, he underwent CT
and MRI scans and a 2M antibodies assay ELISA. Trismus (inability to
open the mouth) was confirmed because it was not possible to open his
mouth even during general anesthesia. MRI revealed severe masticatory
muscle atrophy. ELISA test for 2M antibodies was 1:1000 (reference range
< 1:100), meaning negative for circulating antibodies against
masticatory muscles' 2M fibers.
In
a
September 2022 article, Italian clinicians (Martin Di Tosto,
Carolina Callegari, Kaspar Matiasek, Giuseppe Lacava, Giovanna
Salvatore, Sara Muñoz Declara, Barbara Betti, Federica Tirrito
[right]) report the case study of a 5-month-old male cavalier King
Charles spaniel (in photo below) with an inability to close his
jaw, along with lethargy and difficulty holding food in his mouth
(prehension). He could not close his mouth without assistance, and also
an inability to open his jaw. He also suffered jaw pain, inability to
fully close his eyelids, and atrophy of his masticatory (temporal and
masseter) muscles. In addition to several blood tests and a needle
aspiration of lymph nodes, to eliminate other causes, he underwent CT
and MRI scans and a 2M antibodies assay ELISA. Trismus (inability to
open the mouth) was confirmed because it was not possible to open his
mouth even during general anesthesia. MRI revealed severe masticatory
muscle atrophy. ELISA test for 2M antibodies was 1:1000 (reference range
< 1:100), meaning negative for circulating antibodies against
masticatory muscles' 2M fibers.
Prednisolone was started with a dose of 1 mg/kg every 12 h. After two
weeks of therapy the dog developed
intense
side effects from the glucocorticoids (gastrointestinal signs and severe
high number of neutrophils -- a type of white blood cell -- in the
blood.) So the glucocorticoids were rapidly tapered to 0.5 mg/kg every
24 h for 3 weeks. At follow-up evaluations, clinical signs of MMM and
blood analysis improved: dropped mandible and trismus were no longer
present, food prehension was normal, masticatory muscle atrophy
improved, and creatine kinase and c-reactive protein levels in serum
were within the reference ranges. The dose of prednisolone was gradually
tapered in three months. At three months follow-up, the dog was
clinically stable and treatment with glucocorticoids was stopped. Three
months after treatment, the dog showed a mild relapse of clinical signs
with reluctance to play with a ball due to difficulty in opening the
mouth and mild inappetence. Another course of prednisolone (0.5 mg/kg
every 24 h) for one month duration was completely resolved the clinical
signs. Two months after the last dose of glucocorticoids, the dog did
not present any signs of jaw pain or difficulty in food prehension,
complete blood exams were unremarkable, and neurological examination was
normal with the exception of moderate masticatory muscles atrophy.
May 2017:
Cavalier puppy diagnosed with masticatory muscle myositis is
successfully treated with prednisolone over 6 months.
 In
a
May 2017 article, Drs. Simon Tappin (right), Kate Murphy at
Langford House, UK, report a case of a 4 month old female cavalier King
Charles spaniel with "episodic facial swelling, progressive inability to
open the jaw, and exopthalmia. During these episodes, the masticatory
muscles appeared to swell and became firm and painful." Clinical
examination revealed bilateral swelling of the masseter muscles, slight
bulging of the eyes and discomfort on palpation of the masticatory
muscles. Her jaw opening was limited. Biopsy of the masseter muscles
revealed inflammation, myfiber loss, edema, and fibrosis. (See image
at left.) The dog also was diagnosed with a Neospora infection,
suspected as a trigger for the
In
a
May 2017 article, Drs. Simon Tappin (right), Kate Murphy at
Langford House, UK, report a case of a 4 month old female cavalier King
Charles spaniel with "episodic facial swelling, progressive inability to
open the jaw, and exopthalmia. During these episodes, the masticatory
muscles appeared to swell and became firm and painful." Clinical
examination revealed bilateral swelling of the masseter muscles, slight
bulging of the eyes and discomfort on palpation of the masticatory
muscles. Her jaw opening was limited. Biopsy of the masseter muscles
revealed inflammation, myfiber loss, edema, and fibrosis. (See image
at left.) The dog also was diagnosed with a Neospora infection,
suspected as a trigger for the
 development
of 2M auto-antibodies, which was treated with antibiotics. After 3
weeks, anti-inflammatory doses of prednisolone were added. The dosage
was incrementally increased to an immunosuppressive dose (1mg/kg/BID).
The dog remained stable and the jaw movement increased rapidly over the
next 2 weeks. The prednisolone dose was then gradually reduced over the
next 6 months. The dog continued to have a slight head tilt and the
absence menace response but otherwise has had a very good quality of
life. The dog's jaw opens close to a normal range with normal chewing.
development
of 2M auto-antibodies, which was treated with antibiotics. After 3
weeks, anti-inflammatory doses of prednisolone were added. The dosage
was incrementally increased to an immunosuppressive dose (1mg/kg/BID).
The dog remained stable and the jaw movement increased rapidly over the
next 2 weeks. The prednisolone dose was then gradually reduced over the
next 6 months. The dog continued to have a slight head tilt and the
absence menace response but otherwise has had a very good quality of
life. The dog's jaw opens close to a normal range with normal chewing.
 August
2013:
Italian researchers find MRI can detect early masticatory muscle myositis.
In a September 2013 journal
article, a team of Italian veterinary researchers (Alberto Cauduro
[right],
Favole Paolo, Roberto M. Asperio, Valeria Rossini, Maurizio Dondi, Lucia A.
Simonetto, Carlo Cantile, Valentina Lorenzo)
report that MRIs detected "widespread, symmetrical, and inhomogeneously
hyperintense areas in the masticatory muscle", enabling early diagnosis and
therapeutic treatment."
August
2013:
Italian researchers find MRI can detect early masticatory muscle myositis.
In a September 2013 journal
article, a team of Italian veterinary researchers (Alberto Cauduro
[right],
Favole Paolo, Roberto M. Asperio, Valeria Rossini, Maurizio Dondi, Lucia A.
Simonetto, Carlo Cantile, Valentina Lorenzo)
report that MRIs detected "widespread, symmetrical, and inhomogeneously
hyperintense areas in the masticatory muscle", enabling early diagnosis and
therapeutic treatment."
RETURN TO TOP
Related Links
RETURN TO TOP
Veterinary Resources
Canine muscle fiber types and susceptibility of masticatory muscles to myositis. Julia Stephens Orvis, Dr. George H. Cardinet III. Muscle & Nerve 1981; 4(4):354-359. Quote: "The histopathologic features in temporalis muscle biopsies from 29 dogs with masticatory muscle disorders were characterized and used for their subgrouping: 2 without lesions, 3 with nonspecific changes, 7 with neurogenic atrophy, and 16 with myositis. The immunocytochemical and immunochemical features of the muscle biopsies and sera from those dogs were compared among the histopathologic subgroupings and compared with biopsies and sera from healthy dogs and dogs with polymyositis. Of the 14 biopsies from dogs with masticatory muscle myositis, 12 had immune complexes limited to type 2M fibers, whereas 13 of 16 sera samples had detectable antibodies against type 2M fibers. The immune complex deposition was found only in biopsies of dogs with masticatory muscle myositis, and the antibodies were detected in the sera of only one dog that did not have masticatory muscle myositis. Immunoblot assays revealed that the antibodies were most often directed against a 185 K protein, myosin heavy chain, and a band that appeared to be LC2-M (myosin light chain 2-masticatory)."
Fiber type-specific autoantibodies in a dog with eosinophilic myositis. Dr. G. Diane Shelton, Dr. George H. Cardinet III, Dr. Everett Bandman, Dr. Paul Cuddon. Muscle & Nerve 1985; 8(9): 783-790.
Canine masticatory muscle disorders: A study of 29 cases. Dr. G. Diane Shelton, Dr. George H. Cardinet III, Dr. Everett Bandman. Muscle & Nerve 1987; 10(8):753-766. Quote: The histopathologic features in temporalis muscle biopsies from 29 dogs with masticatory muscle disorders were characterized and used for their subgrouping: 2 without lesions, 3 with nonspecific changes, 7 with neurogenic atrophy, and 16 with myositis. The immunocytochemical and immunochemical features of the muscle biopsies and sera from those dogs were compared among the histopathologic subgroupings and compared with biopsies and sera from healthy dogs and dogs with polymyositis. Of the 14 biopsies from dogs with masticatory muscle myositis, 12 had immune complexes limited to type 2M fibers, whereas 13 of 16 sera samples had detectable antibodies against type 2M fibers. The immune complex deposition was found only in biopsies of dogs with masticatory muscle myositis, and the antibodies were detected in the sera of only one dog that did not have masticatory muscle myositis. lmmunoblot assays revealed that the antibodies were most often directed against a 185 K protein, myosin heavy chain, and a band that appeared to be LC2-M (myosin light chain 2-masticatory).
Masticatory myopathy in the dog: a retrospective study of 18 cases. Gilmour MA, Morgan RV, Moore FM. J Am Anim Hosp Assoc. Jul/Aug 1992; 28(4):300-306. Quote: Eighteen cases of canine masticatory myopathy were reviewed. Case selection was based on clinical signs and muscle biopsy specimens. The majority were under four years of age with no sex, breed, or size predilection. Seventeen of 18 received corticosteroid treatment at various doses. Of the 14 with known responses to therapy, eight (57%) showed complete response, five (36%) a partial response, and one (7%) no response. There was no correlation between the extent or type of pathological lesion and response to therapy. Long-term follow-up was available for nine cases. Eight had no recurrence of signs and normal jaw mobility. One with no initial response to therapy never improved and died one year later.
An Investigation into the Cause and Most Successful Treatment of a Group of Symptoms, Particularly a Stiff Jaw and Swelling Head, in 32 Cases of CKCS. Vera Darby, Anne East. Copyright Vera A. Darby 1995.
Masticatory Muscle Myositis: Pathogenesis, Diagnosis, and Treatment. Caeley Melmed, G. Diane Shelton, Robert Bergman, Claudia Barton. Compendium. Aug. 2004. Quote: "Masticatory muscle myositis is an inflammatory myopathy in which patients most commonly present with jaw pain or an inability to open the jaw. This disease is an autoimmune process in which circulating antibodies specifically target the masticatory muscles. Patients can present either in the acute or, more commonly, chronic phase of the disease. Dogs generally demonstrate no other neurologic or physical abnormalities, which may help differentiate this disease from other causes of trismus. Masticatory muscle myositis requires early detection and aggressive immunosuppressive therapy to improve the prognosis. ... Cavalier King Charles spaniels appear to have a genetic predisposition to masticatory muscle myositis."
Canine Inflammatory Myopathies: A Clinicopathologic Review of 200 Cases. Jason Evans, Donald Levesque, and G. Diane Shelton. J Vet Intern Med 2004;18:679-691. Quote: A retrospective study was performed on 200 randomly selected cases of inflammatory myopathy in dogs from diagnostic muscle biopsies received at the Comparative Neuromuscular Laboratory, University of California, San Diego. The most common clinical signs in dogs diagnosed with an inflammatory myopathy were generalized weakness, stilted gait, dysphagia, masticatory or generalized muscle atrophy, inability to open the jaw, megaesophagus, and dysphonia. Myalgia was rarely described. Age of onset ranged from 0.25 to 14 years. Genders were equally represented. Breed distribution approximated the 2002 American Kennel Club registration statistics (r= .85) with the notable exception of Boxers and Newfoundlands. From the results of muscle biopsies, clinical signs, and presence or absence of antibodies against type 2M fibers, dogs were classified as a generalized inflammatory myopathy (gIM)-ncluding immune-mediated polymyositis; infectious and preneoplastic myositis; and, rarely, dermatomyositislike or overlap syndromes or unclassified myositis-ra focal inflammatory myopathy (fIM)-including masticatory muscle and ex-traocular myositis. Average creatine kinase (CK) and aspartate aminotransferase (AST) concentrations in gIMs were significantly higher than those with fIMs (P < .05). Neoplasia developed in 12 of 200 dogs within 12 months of diagnosis of polymyositis, with lymphoma diagnosed in 6 of 32 Boxers. Inflammatory myopathy was associated with antibody titers against infectious diseases in 38 dogs. Neospora caninum and Hepatozoon americanum cysts were found in tissues of 2 dogs not serologically tested. Antibodies against an unidentified sarcolemmal antigen were found in 9 of 19 Newfoundlands with polymyositis. The spectrum of canine inflammatory myopathies can be broad, with infectious etiologies relatively common, and can include preneoplastic and uncharacterized syndromes.
Masticatory muscle myositis in a young male Cavalier King Charles
Spaniel.
 Dr. Dana Graham. Comparative Neuromuscular
Laboratory at the University of California, San Diego; July 2005. Quote: "The
pup was born 3/15/05. An initial DHPP vaccination was given by the breeder, and
booster DHPP and intranasal Bordatella vaccines were given at 9 weeks of age. At
that time, physical examination was with normal limits with the exception of a
small, reducible umbilical hernia. The dog was also dewormed and placed on
preventative treatment for fleas. Ten days following the second vaccination, the
dog presented for lethargy and anorexia. ... Conclusion by Dr. Diane Shelton: In
a search of the database of the Comparative Neuromuscular Laboratory over the
years 2001-2005, masticatory muscle myositis was confirmed in 11 young Cavalier
King Charles Spaniels with onset at less than 6 months of age. In several cases,
onset followed within 10 days of vaccinations. Although long-term information is
not yet complete, there was resolution of clinical signs of masticatory muscle
myositis in most cases. Of interest, other complications such as early onset
hypothyroidism and allergies were reported. Additional information will be
provided as more is learned about this early-onset masticatory muscle myositis
in this breed."http://vetneuromuscular.ucsd.edu/cases/2017/May.html
Dr. Dana Graham. Comparative Neuromuscular
Laboratory at the University of California, San Diego; July 2005. Quote: "The
pup was born 3/15/05. An initial DHPP vaccination was given by the breeder, and
booster DHPP and intranasal Bordatella vaccines were given at 9 weeks of age. At
that time, physical examination was with normal limits with the exception of a
small, reducible umbilical hernia. The dog was also dewormed and placed on
preventative treatment for fleas. Ten days following the second vaccination, the
dog presented for lethargy and anorexia. ... Conclusion by Dr. Diane Shelton: In
a search of the database of the Comparative Neuromuscular Laboratory over the
years 2001-2005, masticatory muscle myositis was confirmed in 11 young Cavalier
King Charles Spaniels with onset at less than 6 months of age. In several cases,
onset followed within 10 days of vaccinations. Although long-term information is
not yet complete, there was resolution of clinical signs of masticatory muscle
myositis in most cases. Of interest, other complications such as early onset
hypothyroidism and allergies were reported. Additional information will be
provided as more is learned about this early-onset masticatory muscle myositis
in this breed."http://vetneuromuscular.ucsd.edu/cases/2017/May.html
Masticatory muscle myositis and Neospora infection in a 4 month old
female Cavalier King Charles Spaniel. Dr. Simon Tappin
and Dr. Kate Murphy. Comparative Neuromuscular Laboratory at the University of
California, San Diego; March 2006. Quote: Clinical history: A 4 month old
female Cavalier King Charles Spaniel
presented with a 10 day history of episodic facial swelling, progressive
inability to open the jaw, and exopthalmia. During these episodes, the
masticatory muscles appeared to swell and became firm and painful. ...
Physical and Neurological Examination: At presentation the dog was bright,
alert and in fair body condition (weight 5.25Kg, condition score 2/5).
Clinical examination revealed bilateral swelling of the masseter muscles,
slight exophthalmia and discomfort on palpation of the masticatory muscle
group and on retropulsion of both eyes. Jaw opening was limited to 15mm. ...
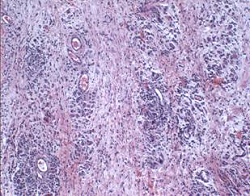
Muscle biopsies: Biopsies were taken from the masseter and temporalis
muscles. These
revealed
multifocal areas of mononuclear cell infiltration composed of scattered
macrophages and clusters of lymphocytes, generalized myofiber loss and
atrophy, fibrosis and edema. (See image at right.)
... Diagnosis and Further Outcome: Supportive care with intravenous fluids
and syringe feeding was initiated and potentiated sulphonamides were also
added (15mg/kg/BID). ... Over the next 4 days the dog's demeanor improved,
the nystamus resolved and the head tilt reduced in severity. The dog was
discharged to her owner at this point. Although the positive 2M antibody
titre confirms a diagnosis of masticatory muscle myositis (MMM), the
positive Neospora IFAT also indicates an active Neospora infection. The
development of acute onset of neurological signs, lead us to believe there
was active Neospora infection within the central nervous system. It was felt
that there may also be Neospora infection within the muscles, however review
of the muscle biopsies in light of this did not reveal any Neospora cysts or
tachyzoites; antibody staining for Neospora was also negative. As
masticatory muscle myositis is an immune mediated condition it is possible
that the Neospora infection acted as a trigger for the development of 2M
auto-antibodies. Masticatory muscle myositis can lead to the rapid
destruction of myofibers and fibrosis, and immunosuppressive therapy with
corticosteroids is indicated. In this case steroids were not added initially
due to the concern of worsening Neospora infection. Six weeks of clindamycin
and potentiated sulphonamides were prescribed, and after 3 weeks,
anti-inflammatory doses of corticosteroids were added. The dosage was
incrementally increased to an immunosuppressive dose (1mg/kg/BID) whilst
watching for worsening of the neurological signs. The dog remained stable
and the jaw movement increased rapidly over the next 2 weeks. The
prednisolone dose was then gradually reduced over the next 6 months.
Outcome: The dog has now completed the 6 month tapering prednisolone course,
and although a slight head tilt and the absence menace response are still
present, the dog has a very good quality of life. The dog's jaw opens close
to a normal range with normal prehension and chewing.
Atypical masticatory muscle myositis in three cavalier King Charles spaniel littermates. Pitcher GD, Hahn CN. J Small Anim Pract. 2007 Apr;48(4):226-8. Quote: This case report describes a novel manifestation of the immune-mediated disease, masticatory muscle myositis. Clinical signs, including difficulty in opening the mouth (trismus), were seen in three of four 12-week-old cavalier King Charles spaniel littermates. ... A litter of four male CKC spaniel puppies were examined and given routine vaccination at eight and 10 weeks of age. Seventeen days later, one of the male puppies (A) was presented with a seven-day history of difficulty in opening the jaw. ... Diagnosis was established by 2M immuno-histochemistry, supported by characteristic histopathological changes in affected temporal muscle. ... Clinical signs included the inability to close the eyelids in two of the puppies. Failure to elicit a blink in testing the palpebral and corneal reflexes and menace response can only be as a result of dysfunction of the facial nerve and/or the orbicularis oculi muscle, which is innervated by the facial nerve and effects the blink response. ... Treatment using corticosteroids at immune-modifying doses resulted in resolution of clinical signs in all the affected animals. ... At follow-up one month later, the ability to open the mouth remained slightly reduced and temporal muscle atrophy had progressed in all the three affected individuals. Whereas dog B was able to close both its eyes normally, the reduced blink response remained in dog A. ... Masticatory muscle myositis should be considered as a differential diagnosis in groups of young dogs with clinical signs of myositis localised to the head. ... It is interesting to speculate that the CKC spaniel may be predisposed to a ''juvenile'' variant of MMM, in which case, further study would be warranted.
A Practical Guide to Canine and Feline Neurology. Curtis W. Dewey. John Wiley & Sons; 2008; 491. Quote: "Most dogs with masticatory myositis are young adults. However, juvenile onset of masticatory myositis has been reported in 12-week-old Cavalier King Charles Spaniel dogs."
Breed Predispositions to Disease in Dogs & Cats (2d Ed.). Alex Gough, Alison Thomas. 2010; Wiley-Blackwell Publ. 52.
Genetic Connection: A Guide to Health Problems in Purebred Dogs, Second Edition. Lowell Ackerman. July 2011; AAHA Press; pg 126. Quote: "Masticatory myositis, also known as eosinphylic myositis and atrophic myositis, is an immune-mediated disease in which antibodies are directed against type II M fibers in masticatory muscles. It is most commonly reported in the German shepherd dog, but other overrepresented breeds include the Cavalier King Charles spaniel ...."
 Imaging
Evaluation of Dogs and Cats with Dysphagia. Rachel E. Pollard. ISRN
Vet. Sci. 2012. Quote: The current literature is reviewed in this paper
regarding the application of diagnostic imaging in the evaluation of
swallowing disorders of the dog. The applications of radiography, contrast
radiography, and contrast videofluoroscopy are discussed with pertinent case
examples provided for emphasis. The indications for image-guided
interventions are also described. ... Figure 7: Digitally captured
fluoroscopic images are shown from a 2-year-old castrated male
Cavalier King Charles Spaniel with pharyngeal weakness related to
immune mediated polymyositis. (a) (at right here) This image is
taken as the dog laps barium that is placed into the mouth using a catheter
tipped syringe but before swallowing is initiated. A small quantity of
barium contrast medium is present in the oral cavity (black arrows) with
some residual barium in the proximal esophagus from the previous swallow
(*). Aspirated barium is also seen in the larynx (LA) and proximal trachea.
UES = upper esophageal sphincter. (b) The dorsal pharyngeal wall (DP)
contracts ventrally to meet the tongue base (TB) but bolus propulsion is
lazy and incomplete. The upper esophageal sphincter (UES) opens in a timely
manner in relation to pharyngeal contraction. (c) After the bolus passes
through the UES and the swallow is complete a moderate quantity of barium
remains in the oral cavity.
Imaging
Evaluation of Dogs and Cats with Dysphagia. Rachel E. Pollard. ISRN
Vet. Sci. 2012. Quote: The current literature is reviewed in this paper
regarding the application of diagnostic imaging in the evaluation of
swallowing disorders of the dog. The applications of radiography, contrast
radiography, and contrast videofluoroscopy are discussed with pertinent case
examples provided for emphasis. The indications for image-guided
interventions are also described. ... Figure 7: Digitally captured
fluoroscopic images are shown from a 2-year-old castrated male
Cavalier King Charles Spaniel with pharyngeal weakness related to
immune mediated polymyositis. (a) (at right here) This image is
taken as the dog laps barium that is placed into the mouth using a catheter
tipped syringe but before swallowing is initiated. A small quantity of
barium contrast medium is present in the oral cavity (black arrows) with
some residual barium in the proximal esophagus from the previous swallow
(*). Aspirated barium is also seen in the larynx (LA) and proximal trachea.
UES = upper esophageal sphincter. (b) The dorsal pharyngeal wall (DP)
contracts ventrally to meet the tongue base (TB) but bolus propulsion is
lazy and incomplete. The upper esophageal sphincter (UES) opens in a timely
manner in relation to pharyngeal contraction. (c) After the bolus passes
through the UES and the swallow is complete a moderate quantity of barium
remains in the oral cavity.
Masticatory Myositis (Eosinophilic Myositis). The Pet Health Care Library. 2013. Quote: "The average patient age is 3 years old. The most common breeds are German shepherds, Labrador retrievers, Doberman pinschers, Golden retrievers, and Cavalier King Charles spaniels. Patients can be of either gender. In the acute phase of the disease, the masticatory muscles are swollen and the eyes appear to bulge due to the swollen pterygoid muscles behind them. There may be a fever and local lymph node swelling at this stage. Results are best if therapy is initiated at this point but unfortunately many owners do not notice the problem until the muscles begin to atrophy and the jaws are rigidly closed, making eating difficult."
Bilateral rastral mandibulectomy for correction of limited mouth opening caused by masticatory muscle myositis: case report in a dog. Arias, M.V.B. et al. MEDVEP. 2013.
Use of MRI for the Early Diagnosis of Masticatory Muscle Myositis. Alberto Cauduro, Favole Paolo, Roberto M. Asperio, Valeria Rossini, Maurizio Dondi, Lucia A. Simonetto, Carlo Cantile, Valentina Lorenzo. J.Am.Anim.Hosp.Assn. Sept. 2013;49(5). Quote: "The medical records of two dogs that were diagnosed with masticatory muscle myositis (MMM) were reviewed. The reported clinical signs included intense pain when opening the mouth and restricted jaw movement. MRI detected widespread, symmetrical, and inhomogeneously hyperintense areas in the masticatory muscle. Electromyography (EMG) demonstrated severe and spontaneous pathologic activity in the temporal and masseter muscles. With early therapeutic treatment, remission of symptoms occurred within 2 mo, and no relapses were observed for the subsequent 2 yr. The gold standard for the diagnosis of MMM is the 2M antibody test, but the purpose of this study was to evaluate the use of MRI as an accurate and efficient diagnostic tool for the initiation of early therapy for the treatment of muscle myositis."
Early Diagnosis of Masticatory Muscle Myositis Is Needed for Treatment Success. Purina ProClub. Jan. 2014. Quote: "Imagine what it would be like if your Golden Retriever could not open his mouth to eat and drink. That is often what happens with an autoimmune disorder called masticatory muscle myositis (MMM) that affects the jaw muscles, causing pain and dysfunction. Swollen, painful masticatory (chewing) muscles and an inability to open the mouth (trismus) are clinical signs of the disorder. 'These dogs are not able to pick up a ball or eat without experiencing severe pain,' says Brian E. Greenfield, D.V.M., who practices at Animal Clinic Northview in North Ridgeville, Ohio. 'In the early stages of the disease, the muscles that are used for eating and chewing appear swollen. As the disease progresses, these muscles begin to atrophy, or waste away. Sometimes the eyes appear sunken, or, less commonly, they seem to protrude.' Although MMM can occur in any breed, it occurs more commonly in large breeds, such as Golden Retrievers, Doberman Pinschers, German Shepherd Dogs, and Labrador Retrievers. Young Cavalier King Charles Spaniels may be severely affected and are believed to be genetically predisposed to developing MMM. Although the disorder does not occur on a widespread basis in Golden Retrievers, anecdotal data suggest that the incidence may be increasing. Thus, whenever a Golden is suddenly unable to open his mouth, experts recommend immediate veterinary care to determine the cause. The condition occurs in males and females, with an average age of onset of 3 years, though puppies as young as 4 months have been affected. Fortunately, if MMM is diagnosed early, dogs can be treated to increase the likelihood of a full recovery. Research of this disease at the University of California-San Diego led to the development of a blood test in 2004 that detects the presence of 2M antibodies and accurately identifies affected dogs.
Treatment Outcome of 22 Dogs With Masticatory Muscle Myositis (1999-2015). Ana C. Castejon-Gonzalez, Maria Soltero-Rivera, Dorothy C. Brown. J. Vet. Dentistry. December 2018;35(4):281-289. Quote: Medical records of dogs diagnosed with masticatory muscle myositis (MMM) at Ryan Veterinary Hospital of the University of Pennsylvania during a period of 17 years (from 1999 to 2015) were reviewed. Twenty-two dogs were included in this retrospective case series study. Immunosuppressive doses of prednisone were prescribed to all dogs. [None were cavalier King Charles spaniels.] Twenty dogs had full recovery of masticatory function. The mean (SD) improvement in the vertical mandibular range of motion (vmROM) was 5.3 (3.1) cm during the first 4 weeks of treatment (weeks 1-4) and 2.8 (2.2) cm during the subsequent 8 weeks (weeks 5-12). The vmROM continued to improve for several more months. Six dogs had a relapse, but the clinical signs were more severe in dogs when no longer receiving prednisone compared to dogs still on prednisone at the time of relapse. When diagnosed and treated appropriately, MMM has a good prognosis with relatively quick return to masticatory function. Early discontinuation of prednisone therapy should be avoided. Approximately 1 year of therapy is recommended prior to discontinuing the medication. Educating the client about how to perform muscle palpation, determine vmROM at home, recognize signs of pain, and notice behavioral changes may help in the early detection of relapses.
Juvenile onset masticatory muscle myositis diagnosed in a 16-week-old Cavalier King Charles Spaniel puppy. Lu Hy. Australian Vet. Pract. December 2019. Quote: A 16-week-old female spayed Cavalier King Charles Spaniel (CKCS) was referred with a 3-day history of dysphagia, hypersalivation, lip-smacking and unwillingness to open the mouth. The puppy's mouth was held slightly open at rest and saliva staining of the fur around the mouth was observed. Pain was elicited on manipulation of the jaw and trismus was exhibited. A mild increase in creatine kinase was present (1190 IU/L; RI 0-385 IU/L) and 2M fibre antibody testing was positive, with a titre of 1:500 mg/dL, confirming the diagnosis of masticatory muscle myositis (MMM). Conclusion: This is the first reported case of MMM in a juvenile CKCS puppy in New Zealand. Together with a previous publication of atypical MMM in three 12-week-old CKCS puppies from the same litter in the UK, and 11 juvenile CKCS identified with MMM in the USA, it reinforces the prevalence of MMM in young CKCS puppies and again raises the hypothesis of MMM being a genetically predisposed disease in the breed.
Case report: Atypical and chronic masticatory muscle myositis in a 5-month old Cavalier King Charles Spaniel. Clinical and diagnostic findings, treatment and successful outcome. Martin Di Tosto, Carolina Callegari, Kaspar Matiasek, Giuseppe Lacava, Giovanna Salvatore, Sara Muñoz Declara, Barbara Betti, Federica Tirrito. Front. Vet. Sci. September 2022; doi: 10.3389/fvets.2022.955758. Quote: Masticatory muscle myositis (MMM) is the second most common inflammatory myopathy diagnosed in dogs, but it is rarely described in puppies. The disease is characterized by the production of autoantibodies against 2M myofibers contained in masticatory muscle, although the cause of this production is still unclear. The aim of the present case report was to describe the clinical presentation, diagnostic findings, treatment, and follow-up of an atypical case of chronic masticatory muscle myositis in a very young dog. A 5-month old Cavalier king Charles Spaniel (CKCS) was presented to the AniCura Istituto Veterinario Novara with a two weeks, progressive history of lethargy and difficulty in food prehension. Neurological examination revealed bilateral masticatory muscle atrophy, mandibular ptosis with the jaw kept open, inability to close the mouth without manual assistance, jaw pain, and bilateral reduction of palpebral reflex and menace reaction; vision was maintained. A myopathy was suspected. Computed tomography (CT), magnetic resonance imaging (MRI), enzyme-linked immunosorbent assay test for 2M antibodies, and histopathological examination of masticatory muscle biopsy confirmed the diagnosis of MMM. ... ELISA test for 2M antibodies was 1:1000 (reference range < 1:100). ... Prednisolone was started with a dose of 1 mg/kg every 12 h. After two weeks of therapy the dog developed intense glucocorticoids associated side effects (i.e., gastrointestinal signs and severe neutrophilic leucocytosis); for this reason, glucocorticoids were rapidly tapered to 0.5 mg/kg every 24 h and this dose was continued for 3 weeks. At follow-up evaluations, clinical signs of MMM and blood analysis improved: dropped mandible and trismus were no longer present, food prehension was normal, masticatory muscle atrophy improved, and creatine kinase and c-reactive protein levels in serum were within reference range. The dose of prednisolone was further gradually tapered in three months. At three months follow-up, the dog was clinically stable and treatment with glucocorticoids was interrupted. Three months after treatment, the dog showed a mild relapse of clinical signs with reluctance to play with a ball due to difficulty in opening the mouth and mild inappetence; a course of prednisolone (0.5 mg/kg every 24 h) of one month duration was effective in complete resolution of clinical signs. Two months after the last administration of glucocorticoids, the dog did not present any signs of jaw pain or difficulty in food prehension, complete blood exams were unremarkable, and neurological examination was normal with the exception of moderate masticatory muscles atrophy. ... [T]o the authors' knowledge, this is the first report describing a dropped mandible in a case of confirmed MMM. ... In the present case, glucocorticoids treatment allowed a significant clinical improvement, despite the signs of chronic inflammation. The dog was able to completely open its mouth and most of the masticatory muscle trophism recovered. ... To the authors' knowledge, this is the first case describing mandibular ptosis in a dog affected by chronic MMM, successfully managed with medical treatment and the first report describing the CT and MRI findings in a young CKCS affected by MMM. ... Young CKCSs with MMM might have a good prognosis with rapid and marked improvement with glucocorticoid treatment, even if presented with signs of chronicity.
CONNECT WITH US